
Skeletal Muscle Relaxants Drugs
Skeletal Muscle Relaxants
- The main clinical use of skeletal muscle relaxant is it acts an adjuvant in surgical anesthesia to obtain relaxation of skeletal muscles à this minimizes the risk of respiratory & cardiovascular depression
- These drugs block the post-synaptic actions of ACh at motor end plate
- On the basis of their site & mechanism of action…these are classified as
- Peripherally acting muscle relaxants[These act peripherally at neuromuscular junction]
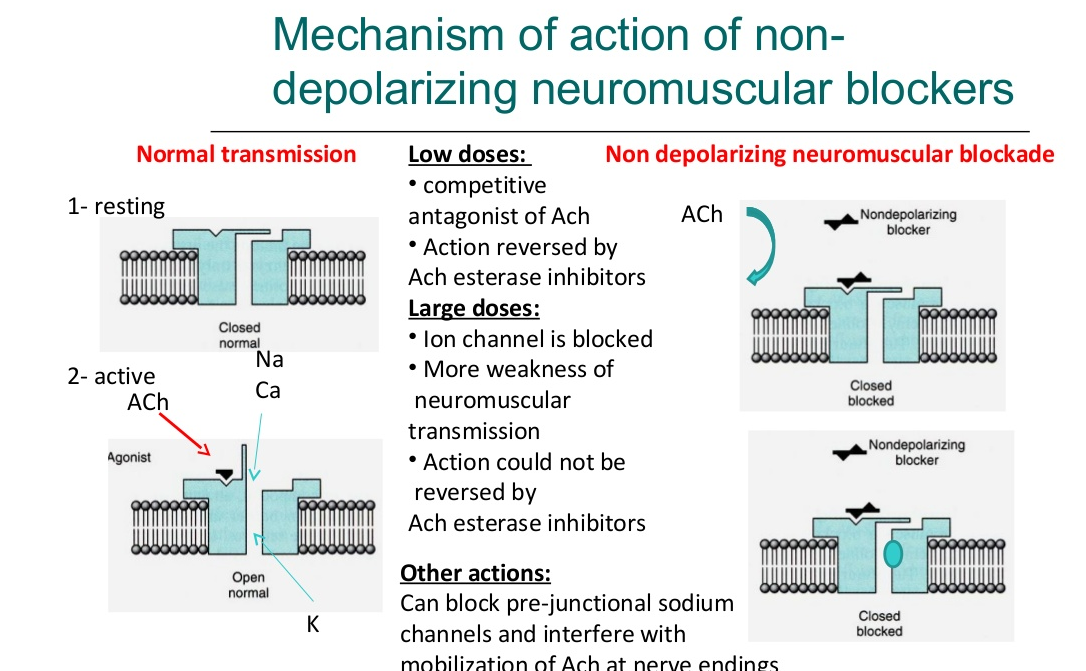
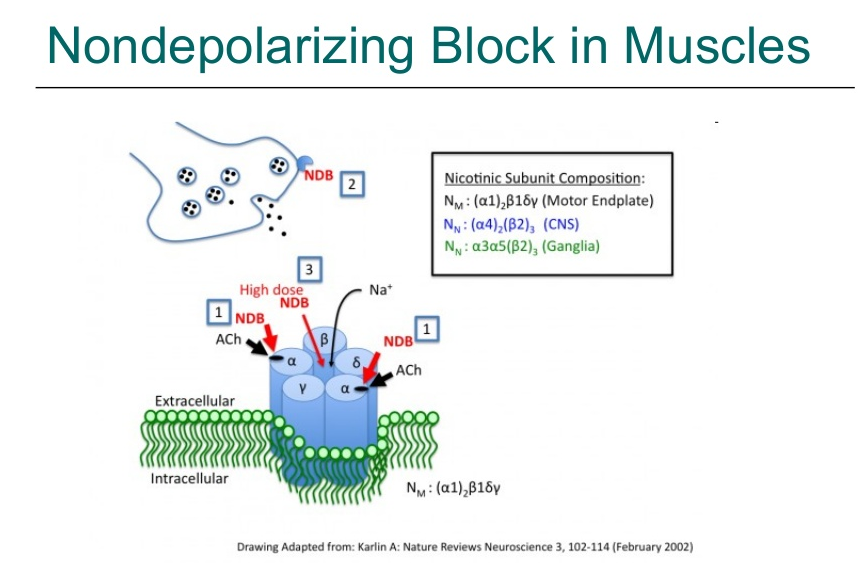
- a) Non-Depolarizing Blockers (Competitive Blockers)
- Basis:These drugs prevent the access of ACh to NM receptor of motor end plate à prevent its depolarization
- Long Acting: d-Tubocurarine (d-TC), Metocurine, Doxacurium, pancuronium, pipecuronium, gallamine
- Intermediate acting: Atracurium, Cisatracurium, Vecuronium, Rcuronium
d-Tubocurarine: – Not clinical used do to its histaminic effects. • Succinylcholine: – SCh is the most commonly used muscle relaxant for passing tracheal tube. It induces rapid, complete and predictable paralysis with spontaneous recovery in ~5 min. – Occasionally SCh is used by continuous i.v. infusion for producing controlled muscle relaxation of longer duration. – It should be avoided in younger children unless absolutely necessary, because risk of hyperkalaemia and cardiac arrhythmia is higher
Pancuronium: – It is a synthetic steroidal compound, ~5 times more potent and longer acting than d-TC. – Because of longer duration of action, needing reversal, its use is now restricted to prolonged operations, especially neurosurgery. • Pipecuronium: – Muscle relaxant with a slow onset and long duration of action; steroidal in nature; recommended for prolonged surgeries. Nondepolarizing blockers – Individual compounds
Vecuronium: – It is a most commonly used muscle relaxant for routine surgery and in intensive care units.. • Atracurium: – Four times less potent than pancuronium and shorter acting. • Rocuronium: – Muscle relaxant with a rapid onset and intermediate duration of action which can be used as alternative to SCh for tracheal intubation without the disadvantages of depolarizing block and cardiovascular changes. Nondepolarizing blockers – Individual compounds
iii. Short Acting: Mivacurine, Rapacuronium
- b) Depolarizing Blockers (persistent depolarizers)
- Basis:They produce an excessive depolarization which persists for longer duration at NMJ à because they are resistant to hydrolysis by true AChE present in synaptic cleft
- Succinyl Choline
-
Centrally Acting Muscle Relaxants
- Basis:These drugs reduce skeletal muscle tone à by selective action in the cerebrospinal axis without altering consciousness
- Carisoprodol, Chlorzoxazone, Diazepam, Clonazepam, Baclofen, Tizanidine
III. Directly Acting Muscle Relaxants
- Basis:These directly interfere with the contractile mechanisms of voluntary muscle
- Dantrolene
- Misc Group
- Quinine, Botulinum toxins A & B
Comparison of d-Tubocurarine & Succinylcholine
| Parameters | d-Tubocurarine | Succinylcholine |
| 1.Mechanism | Competitive blockade at NM receptors | Persistent depolarization of NM receptors followed by their desensitization |
| 2.Potency | ++ (Moderate) | + (less) |
| 3.Onset | 4-5 min | 1 min |
| 4.Duration | 30 – 50 min with no muscle sore | 5 – 6 min followed by muscle sore |
| 5.Type of Relaxation | Progressive flaccid paralysis | Initial fasciculations followed by flaccid paralysis |
| 6.Effect of Neostigmine | Reversal i.e antagonism | Potentiation on effect |
| 7.NM blocking drugs | Potentiation on effect | No effect |
| 8.Hypothermia | Decreases effect | Increased effect |
| 9.Histamine release | ++ (Moderate) | Negligible |
| 10. BP | Hypotension | No effect |
| 11. Cardiac Muscarinic receptors | No effect | Stimulates. Bradycardia in low doses, tachycardia in large doses |
| 12. Respiratory effects | Bronchospasm | Nil |
| 13. GIT Effects | Constipation | Nausea, Vomitting |
| 14. Serum K+ levels | No change | Hyperkalaemia |
| 15. Intraocular pressure | No change | Raised |
| 16. Pharmacogenetic variation in metabolism | Nil (it is excreted through kidney) | Metabolized by pseudocholinesterase (exhibit prolonged apnoea) |
| 17. Other | Nil | Malignanat hyperthermia |
Mechanism of Action of Skeletal Muscle Relaxants Drugs:
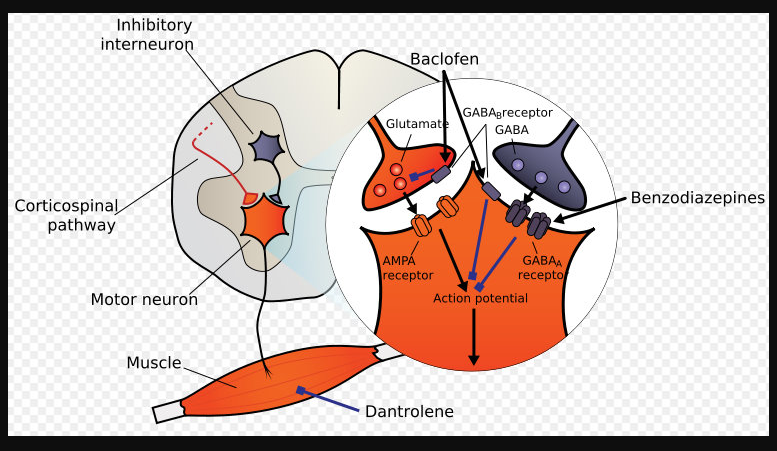



Baclofen
- It is orally active GABA-mimetic drug àwhich acts as a GABA agonist at GABAB receptors
- The GABABreceptors are G-protein coupled receptors à which hyperpolarize neurons by increasing K+ conductance & reduce Ca+2 conductance
- Its actions àresults from an action at spinal level where it inhibits both monosynaptic & polysynaptic reflexes
- Activation of GABAB recptors in the brain àresults in hyperpolarisation in the cord & brain à which interfere with the release of excitatory neurotransmitters
- It also reduces pain associated with spastic conditions ßas it inhibits the release of substance-P in the spinal cord
Baclofen Therapeutic Uses
- To relieve painful spasticity in multiple sclerosis
- It is also used to relieve spasticity from spinal injuries but it is not very useful in cerebral palsy
- It can also serve as an important substitute to treat trigeminal neuralgia & tardive dyskinesia
- It imrves he quality f life of patients suffering with severe spasticity & pain
Baclofen Side Effects
- Sedation, drowsiness, muscle weakness, ataxia
- Sudden withdrawal may precipitate anxiety, tachycardia & Hallucinations
- It is teratogenic & risk in pregnancy
Dantrolene
- It is a phenytoin analogue àbut its site for antispastic action lies ouside the CNS
- It acts directly at the contractile mechanisms of voluntary muscle by reducing depolarization induced Ca+2 release from the sarcoplasmic reticulum
- The muscle fibers still respond to nerve stimulus àthe contractile responses are reduced but not absolutely abolished by dantrolene à the net result is muscle weakness rather than paralysis
- It also facilitates GABA which results in the depression of brain stem reticular functions & efferent motor neuron activity àit produces sedation but no selective action on polysynaptic reflexes
Dantrolene Therapeutic Uses
- It is used to treat spasticity resulting from upper motor neuron lesions such as spinal cord injury, multiple sclerosis & cerebral palsy
- It is the drug of choice for the treatment of malignant hyperthermia
- It is also used in the treatment of neurolept malignant syndrome
- Orally it is poorly absorbed but absorption is consistent
- Plasma half-life is 9-12 hrs
- A/Es– generalized muscle weakness, sedation, diarrhea, hepatitis after prolonged use
References •
Tripathi KD. Essentials of Medical Pharmacology, 7th Ed, New Delhi: Jaypee Brothers Medical Publisher (P) Ltd, 2013.